
|
帕立骨化醇是一种选择性、第3代维生素D受体激活剂。商品名Zemplar,原研公司雅培,其活性成分帕立骨化醇的注射制剂于1998年4月17日由雅培公司在美国首次获准上市,用于预防和治疗与慢性肾病(现在指接受血液透析的慢性肾病患者)相关的继发性甲状旁腺功能亢进症,并于2002年9月在欧盟国家获得上市许可。
Dose Titration Dosing must be individualised based on serum or plasma iPTH levels, with monitoring of serum calcium and serum phosphorus. Table 2 presents a suggested approach for dose titration. Table 2. Dose Titration
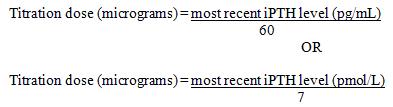
2 If a patient is taking the lowest dose on the daily or three times a week regimen, and a dose reduction is needed, dosing frequency can be decreased. Serum calcium levels should be closely monitored after initiation of the treatment and during dose titration periods. If hypercalcemia or a persistently elevated calcium- phosphate product greater than 55 mg2/dL2 (4.4 mmol2 /L2) is observed, the dose of calcium based phosphate binders should be reduced or withheld. Alternatively, the dose of Zemplar may be reduced or temporarily interrupted. If interrupted, the drug should be restarted at a lower dose, when serum calcium and calcium- phosphate product are in the target range. Chronic Kidney Disease (CKD), Stage 5 Zemplar should be administered three times a week every other day. Initial Dose The initial dose of Zemplar in micrograms is based on a baseline iPTH level (pg/mL)/60 [(pmol/L)/7], up to an initial maximum dose of 32 micrograms. Dose Titration Subsequent dosing should be individualised and based on iPTH, serum calcium and phosphorus levels. A suggested dose titration of paricalcitol capsules is based on the following formula:
The safety of paricalcitol capsules has been evaluated in one 12-week, double-blind, placebo-controlled, multi-centre clinical trial involving 88 CKD Stage 5 patients. There were no statistically significant differences between the paricalcitol-treated patients and placebo-treated patients in the incidence of hypercalcaemia Zemplar (1/61, 2%) vs placebo (0/26, 0.0%), or elevated calcium phosphate product Zemplar (6/61, 10%) vs placebo (1/26, 4%). All adverse events at least possibly related to paricalcitol, both clinical and laboratory, are displayed in Table 4 by MedDRA System Organ Class, Preferred Term and frequency. The following frequency groupings are used: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). Table 4. Adverse Reactions Reported in Stage 5 CKD pivotal phase III Study
Reporting of suspected adverse reactions Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard. 4.9 Overdose Excessive administration of Zemplar capsules can cause hypercalcaemia, hypercalciuria, hyperphosphataemia, and over suppression of parathyroid hormone. High intake of calcium and phosphate concomitant with Zemplar capsules may lead to similar abnormalities. Treatment of patients with clinically significant hypercalcaemia consists of immediate dose reduction or interruption of paricalcitol therapy and includes a low calcium diet, withdrawal of calcium supplements, patient mobilisation, attention to fluid and electrolyte imbalances, assessment of electrocardiographic abnormalities (critical in patients receiving digitalis), and haemodialysis or peritoneal dialysis against a calcium-free dialysate, as warranted. Signs and symptoms of vitamin D intoxication associated with hypercalcaemia include: Early: Weakness, headache, somnolence, nausea, vomiting, dry mouth, constipation, muscle pain, bone pain and metallic taste. Late: Anorexia, weight loss, conjunctivitis (calcific), pancreatitis, photophobia, rhinorrhoea, pruritis, hyperthermia, decreased libido, elevated BUN, hypercholesterolaemia, elevated AST and ALT, ectopic calcification, hypertension, cardiad arrhythmias, somnolence, death and rarely, overt psychosis. Serum calcium levels should be monitored frequently until normocalcaemia ensues. Paricalcitol is not significantly removed by dialysis. 5. Pharmacological properties 5.1 Pharmacodynamic properties Pharmacotherapeutic group: Anti-parathyroid agents –ATC code: H05BX02. Mechanism of Action Paricalcitol is a synthetic, biologically active vitamin D analog of calcitriol with modifications to the side chain (D2) and the A (19-nor) ring. Unlike calcitriol, paricalcitol is a selective vitamin D receptor (VDR) activator. Paricalcitol selectively upregulates the VDR in the parathyroid glands without increasing VDR in the intestine and is less active on bone resorption. Paricalcitol also upregulates the calcium sensing receptor in the parathyroid glands. As a result, paricalcitol reduces parathyroid hormone (PTH) levels by inhibiting parathyroid proliferation and decreasing PTH synthesis and secretion, with minimal impact on calcium and phosphorus levels, and can act directly on bone cells to maintain bone volume and improve mineralization surfaces. Correcting abnormal PTH levels, with normalisation of calcium and phosphorus homeostasis, may prevent or treat the metabolic bone disease associated with chronic kidney disease. Clinical Efficacy Chronic Kidney Disease, Stages 3-4 The primary efficacy endpoint of at least two consecutive ≥ 30 % reductions from baseline iPTH was achieved by 91% of paricalcitol capsules-treated patients and 13% of the placebo patients (p<0.001). Serum bone specific alkaline phosphatase like serum osteocalcin were significantly reduced (p<0.001) in patients treated with paricalcitol capsules compared to placebo, which is associated with a correction of the high bone turnover due to secondary hyperparathyroidism. No deterioration in the kidney function parameters of estimated glomerular filtration rate (via MDRD formula) and serum creatinine was detected in paricalcitol capsules treated patients in comparison to placebo treated patients. Significantly more of paricalcitol capsules treated patients experienced a reduction in urinary protein, as measured by semiquantitative dipstick, compared to placebo treated patients. Chronic kidney disease, Stage 5 The primary efficacy endpoint of at least two consecutive ≥ 30 % reductions from baseline iPTH was achieved by 88% of paricalcitol capsules treated patients and 13% of the placebo patients (p < 0.001). Paediatric clinical data with Zemplar Injection (IV) The safety and effectiveness of Zemplar IV were examined in a 12-week randomised, double-blind, placebo-controlled study of 29 pediatric patients, aged 5-19 years, with end-stage renal disease on hemodialysis. The six youngest Zemplar IV-treated patients in the study were 5 - 12 years old. The initial dose of Zemplar IV was 0.04 mcg/kg 3 times per week, based on baseline iPTH level of less than 500 pg/mL, or 0.08 mcg/kg 3 times a week based on baseline iPTH level of ≥ 500 pg/mL, respectively. The dose of Zemplar IV was adjusted in 0.04 mcg/kg increments based on the levels of serum iPTH, calcium, and Ca x P. 67% of the Zemplar IV-treated patients and 14% placebo-treated patients completed the trial. 60% of the subjects in the Zemplar IV group had 2 consecutive 30% decreases from baseline iPTH compared with 21% patients in the placebo group. 71% of the placebo patients were discontinued due to excessive elevations in iPTH levels. No subjects in either the Zemplar IV group or placebo group developed hypercalcaemia. No data are available for patients under the age of 5. 5.2 Pharmacokinetic properties Absorption Paricalcitol is well absorbed. In healthy subjects, following oral administration of paricalcitol at 0.24 micrograms/kg, the mean absolute bioavailability was approximately 72%; the maximum plasma concentration (Cmax) was 0.630 ng/mL (1.512 pmol/mL) at 3 hours and area under the concentration time curve (AUC0-∞) was 5.25 ng•h/mL (12.60 pmol•h/mL). The mean absolute bioavailability of paricalcitol in hemodialysis (HD) and peritoneal dialysis (PD) patients is 79% and 86%, respectively, with the upper bound of 95% confidence interval of 93% and 112%, respectively. A food interaction study in healthy subjects indicated that the Cmax and AUC0-∞ were unchanged when paricalcitol was administered with a high fat meal compared to fasting. Therefore, Zemplar Capsules may be taken without regard to food. The Cmax and AUC0-∞ of paricalcitol increased proportionally over the dose range of 0.06 to 0.48 micrograms/kg in healthy subjects. Following multiple dosing, either as daily or three times a week in healthy subjects, steady-state exposure was reached within seven days. Distribution Paricalcitol is extensively bound to plasma proteins (> 99%). The ratio of blood paricalcitol to plasma paricalcitol concentration averaged 0.54 over the concentration range of 0.01 to 10 ng/mL (0.024 to 24 pmol/mL) indicating that very little drug associated with blood cells. The mean apparent volume of distribution following a 0.24 micrograms/kg dose of paricalcitol in healthy subjects was 34 litres. Biotransformation After oral administration of a 0.48 micrograms/kg dose of 3H-paricalcitol, parent drug was extensively metabolised, with only about 2% of the dose eliminated unchanged in the faeces, and no parent drug found in the urine. Approximately 70% of the radioactivity was eliminated in the faeces and 18% was recovered in the urine. Most of the systemic exposure was from the parent drug. Two minor metabolites, relative to paricalcitol, were detected in human plasma. One metabolite was identified as 24(R)-hydroxy paricalcitol, while the other metabolite was unidentified. The 24(R)-hydroxy paricalcitol is less active than paricalcitol in an in vivo rat model of PTH suppression. In vitro data suggest that paricalcitol is metabolised by multiple hepatic and non-hepatic enzymes, including mitochondrial CYP24, as well as CYP3A4 and UGT1A4. The identified metabolites include the product of 24(R)-hydroxylation, as well as 24,26- and 24,28-dihydroxylation and direct glucuronidation. Elimination In healthy subjects, the mean elimination half-life of paricalcitol is five to seven hours over the studied dose range of 0.06 to 0.48 micrograms/kg. The degree of accumulation was consistent with the half-life and dosing frequency. Haemodialysis procedure has essentially no effect on paricalcitol elimination. Special Populations Elderly The pharmacokinetics of paricalcitol have not been investigated in patients greater than 65 years. Paediatric The pharmacokinetics of paricalcitol have not been investigated in patients less than 18 years of age. Gender The pharmacokinetics of paricalcitol following single doses over 0.06 to 0.48 micrograms/kg dose range were gender independent. Hepatic Impairment In a study performed with Zemplar intravenous, the disposition of paricalcitol (0.24 micrograms/kg) was compared in patients with mild (n = 5) and moderate (n = 5) hepatic impairment (in accordance with the Child-Pugh method) and subjects with normal hepatic function (n = 10). The pharmacokinetics of unbound paricalcitol was similar across the range of hepatic function evaluated in this study. No dosing adjustment is required in patients with mild to moderate hepatic impairment. The influence of severe hepatic impairment on the pharmacokinetics of paricalcitol has not been evaluated. Renal Impairment Paricalcitol pharmacokinetics following single dose administration were characterised in patients with CKD Stage 3 or moderate renal impairment (n = 15, GFR = 36.9 to 59.1 mL/min/1.73 m2), CKD Stage 4 or severe renal impairment (n = 14, GFR = 13.1 to 29.4 mL/min/1.73 m2), and CKD 5 or end-stage renal disease [n = 14 in haemodialysis (HD) and n = 8 in peritoneal dialysis (PD)]. Similar to endogenous 1,25(OH)2 D3, the pharmacokinetics of paricalcitol following oral administration were affected significantly by renal impairment, as shown in Table 5. Compared to healthy subjects results obtained, Chronic Kidney Disease, Stage 3, 4, and 5 patients showed decreased CL/F and increased half-life. Table 5. Comparison of Mean ± SD Pharmacokinetic Parameters in Different Stages of Renal Impairment versus Healthy Subjects
Following oral administration of paricalcitol capsules, the pharmacokinetic profile of paricalcitol for Chronic kidney disease, Stages 3 to 5 was comparable. Therefore, no special dosing adjustments are required other than those recommended (see section 4.2). 5.3 Preclinical safety data Salient findings in the repeat-dose toxicology studies in rodents and dogs were generally attributed to paricalcitol's calcaemic activity. Effects not clearly related to hypercalcaemia included decreased white blood cell counts and thymic atrophy in dogs, and altered APTT values (increased in dogs, decreased in rats). WBC changes were not observed in clinical trials of paricalcitol. Paricalcitol did not affect fertility in rats and there was no evidence of teratogenic activity in rats or rabbits. High doses of other vitamin D preparations applied during pregnancy in animals lead to teratogenesis. Paricalcitol was shown to affect fetal viability, as well as to promote a significant increase of peri-natal and post-natal mortality of newborn rats, when administered at maternally toxic doses. Paricalcitol did not exhibit genotoxic potential in a set of in-vitro and in-vivo genotoxicity assays. Carcinogenicity studies in rodents did not indicate any special risks for human use. Doses administered and/or systemic exposures to paricalcitol were slightly higher than therapeutic doses/systemic exposures. 6. Pharmaceutical particulars 6.1 List of excipients Capsule contents: Medium chain triglycerides Ethanol Butylhydroxytoluene Capsule shell: 2 microgram Gelatin Glycerol Water Titanium dioxide (E171) Iron oxide red (E172) Iron oxide yellow (E172) Black Ink: Propylene glycol Black iron oxide (E172) Polyvinyl acetate phthalate Macrogol 400 Ammonium hydroxide 6.2 Incompatibilities Not applicable. 6.3 Shelf life 2 years 6.4 Special precautions for storage This medicinal product does not require any special storage conditions. 6.5 Nature and contents of container High-density polyethylene (HDPE) bottles closed with child-resistant polypropylene caps. Each bottle contains 30 capsules. PVC/fluoropolymer/aluminium blister strips containing 7 capsules. Each carton contains 1 or 4 blister strips. Packaged in outer cartons containing either 7 or 28 capsules. Not all pack sizes may be marketed. 6.6 Special precautions for disposal and other handling No special requirements. 7. Marketing authorisation holder AbbVie Ltd., Abbott House Vanwall Business Park Vanwall Road Maidenhead Berkshire SL6 4XE United Kingdom 8. Marketing authorisation number(s) PL 41042/0012 9. Date of first authorisation/renewal of the authorisation 20 January 2012 10. Date of revision of the text 09 May 2014 ------------------------------------------------ 产地国家: 德国 原产地英文商品名: ZEMPLAR 1MCG/CAP 28CAPS/BOTTLE 原产地英文药品名: PARICALCITOL 中文参考商品译名: ZEMPLAR 1微克/胶囊 28胶囊/盒 中文参考药品译名: 帕立骨化醇 生产厂家中文参考译名: ABBVIE 生产厂家英文名: ABBVIE ------------------------------------------------ 产地国家: 德国 原产地英文商品名: ZEMPLAR 2MCG/CAP 28CAPS/BOTTLE 原产地英文药品名: PARICALCITOL 中文参考商品译名: ZEMPLAR 2微克/胶囊 28胶囊/盒 中文参考药品译名: 帕立骨化醇 生产厂家中文参考译名: ABBVIE 生产厂家英文名: ABBVIE | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Zemplar Capsules(PARICALCITOL)帕立骨化醇软胶囊简介:
帕立骨化醇是一种选择性、第3代维生素D受体激活剂。商品名Zemplar,原研公司雅培,其活性成分帕立骨化醇的注射制剂于1998年4月17日由雅培公司在美国首次获准上市,用于预防和治疗与慢性肾病(现在指接受 ... 责任编辑:admin
|
最新文章更多推荐文章更多热点文章更多
|
中国新特药网-第一时间提供全球医药资讯
注: 本站药品信息仅供医药研发机构作参考-
在线咨询:
- 鲁ICP备05035203号 @