|
英文药名: Onbrez(Indacaterol Breezhaler)
中文药名: 马来酸茚达特罗胶囊粉雾剂(吸入)
生产厂家:德国Novartis
药品介绍:
诺华公司(Novartis)的indacaterol(又称QAB149)是一日1次的支气管扩张药,目前本品用于治疗慢性阻塞性肺疾病COPD的上市申请正在接受FDA审批。诺华公司在2008年12月向美国FDA递交了本品的上市申请。据了解,慢性阻塞性肺疾病COPD是诺华公司主要关注的疾病领域,公司希望本品能成为其研发慢性阻塞性肺疾病COPD联合疗法的基础。这些联合疗法包括:用于治疗COPD和哮喘的QMF149(indacaterol + 肾上腺皮质类固醇莫米松),以及用于治疗慢性阻塞性肺疾病COPD的QVA149(indacaterol + 抗毒蕈碱NVA237)。
诺华公司在2005年4月通过产品许可途径获得了由生物技术企业Sosei集团(Sosei Group)和Vectura集团(Vectura Group)合作研发的NVA237。诺华公司计划将NVA237开发为慢性阻塞性肺疾病COPD单一疗法药物:一日1次的长效毒蕈碱拮抗剂(LAMA);以及慢性阻塞性肺疾病COPD联合疗法药物:将NVA237与一日1次的长效β2激动剂(LABA)indacaterol联用。尽管COPD没有彻底治愈的方法,然而LABA和LAMA等支气管扩张剂可以有效缓解疾病症状,是国际治疗手册中的慢性阻塞性肺疾病COPD主要治疗药物。
2009年12月,本品及其吸入装置Concept-1获得欧盟批准用于慢性阻塞性肺疾病COPD患者气道扩张,商品名为Onbrez Breezhaler。Onbrez Breezhaler(indacaterol maleate)为一日1次的定量吸入剂,其中活性成分indacaterol maleate为欧盟7年来首个批准用于慢性阻塞性肺疾病COPD治疗的新化合物。Onbrez Breezhaler是目前第一个也是唯一一个经临床研究证实通过5分钟吸入给药可保持24小时支气管扩张作用的治疗药物。
与此同时,诺华公司2009年10月收到FDA回复函要求提供更多的本品研究资料。诺华方面表示,扩大的Ⅲ期临床研究显示,本品与目前临床常用的噻托溴铵(tiotropium bromide,Spiriva)等支气管扩张剂相比,在改善肺功能和慢性阻塞性肺疾病COPD症状(尤其是气喘)方面具有统计学优势。一项纳入30个国家4400多例患者的Ⅲ期临床研究显示,与现有福莫特罗(formoterol)和tiotropium疗法相比,本品可显著改善肺功能。本品在慢性阻塞性肺疾病COPD治疗中可改善患者的症状控制。据了解,以福莫特罗为主要成分的产品Foradil已于2001年5月在美国上市,本品由诺华公司(Novartis)和先灵葆雅公司(Schering-Plough)共同推广,2008年销售额达到4.89亿美元。另一个以福莫特罗为主要成分的产品是阿斯利康公司(AstraZeneca)的复方平喘药布地奈德+福莫特罗的复方制剂(budesonide+formoterol,Symbicort),该产品2008年销售额达到20亿美元。
慢性阻塞性肺疾病COPD可削弱肺功能,导致慢性气喘,对患者的工作和生活产生诸多不利影响。目前全球范围内大约有2.10亿人受到COPD的困扰,其中大多数是65岁以下人群。本品具有良好的有效性和安全性,而且减少了患者的用药频率,在慢性阻塞性肺疾病COPD治疗领域具有相当的治疗优势。本品最初作为单一疗法上市,然而分析师认为,本品的未来商业潜力将通过其各种复方制剂来实现,预计本品销售额最高可达到30亿~50亿美元。诺华公司与先灵葆雅公司(Schering-plough)显然也意识到了这一点。2009年5月,诺华与先灵葆雅公司就呼吸系统药物全球合作研发计划进行调整。诺华公司拥有COPD和哮喘治疗药在研产品QMF149(indacaterol + 肾上腺皮质类固醇莫米松)的全球研发和商业化权利。据了解,双方在这方面的合作可追溯至2002年,2006年8月进一步扩大,此次调整在销售版税划分方面进行了协商。

Onbrez Breezhaler 150 and 300 microgram inhalation powder, hard capsules
1. Name of the medicinal product
Onbrez Breezhaler 150 microgram inhalation powder, hard capsules
Onbrez Breezhaler 300 microgram inhalation powder, hard capsules
2. Qualitative and quantitative composition
Onbrez Breezhaler 150 microgram inhalation powder, hard capsules:
Each capsule contains indacaterol maleate equivalent to 150 microgram indacaterol.
The delivered dose leaving the mouthpiece of the Onbrez Breezhaler inhaler is indacaterol maleate equivalent to 120 microgram indacaterol.
Excipients:
Each capsule contains 24.8 mg lactose.
Onbrez Breezhaler 300 microgram inhalation powder, hard capsules:
Each capsule contains indacaterol maleate equivalent to 300 microgram indacaterol.
The delivered dose leaving the mouthpiece of the Onbrez Breezhaler inhaler is indacaterol maleate equivalent to 240 microgram indacaterol.
Excipients:
Each capsule contains 24.6 mg lactose.
For the full list of excipients, see section 6.1.
3. Pharmaceutical form
Inhalation powder, hard capsule
Onbrez Breezhaler 150 microgram inhalation powder, hard capsules:
Clear colourless capsules containing a white powder, with “IDL 150” printed in black above and company logo () printed in black below a black bar.
Onbrez Breezhaler 300 microgram inhalation powder, hard capsules:
Clear colourless capsules containing a white powder, with “IDL 300” printed in blue above and company logo () printed in blue below a blue bar.
4. Clinical particulars
4.1 Therapeutic indications
Onbrez Breezhaler is indicated for maintenance bronchodilator treatment of airflow obstruction in adult patients with chronic obstructive pulmonary disease (COPD).
4.2 Posology and method of administration
Posology
The recommended dose is the inhalation of the content of one 150 microgram capsule once a day, using the Onbrez Breezhaler inhaler. The dose should only be increased on medical advice.
The inhalation of the content of one 300 microgram capsule once a day, using the Onbrez Breezhaler inhaler has been shown to provide additional clinical benefit with regard to breathlessness, particularly for patients with severe COPD. The maximum dose is 300 microgram once daily.
Onbrez Breezhaler should be administered at the same time of the day each day.
If a dose is missed the next dose should be taken at the usual time the next day.
Elderly population
Maximum plasma concentration and overall systemic exposure increase with age but no dose adjustment is required in elderly patients.
Paediatric population
There is no relevant use of Onbrez Breezhaler in the paediatric population (under 18 years).
Hepatic impairment
No dose adjustment is required for patients with mild and moderate hepatic impairment. There are no data available for use of Onbrez Breezhaler in patients with severe hepatic impairment.
Renal impairment
No dose adjustment is required for patients with renal impairment.
Method of administration
For inhalation use only. Onbrez Breezhaler capsules must not be swallowed.
Onbrez Breezhaler capsules must be administered only using the Onbrez Breezhaler inhaler (see section 6.6)
Patients should be instructed on how to administer the product correctly. Patients who do not experience improvement in breathing should be asked if they are swallowing the medicine rather than inhaling it.
For instructions on use of the medicinal product before administration, see section 6.6.
4.3 Contraindications
Hypersensitivity to the active substance, to lactose or to any of the other excipients listed in section 6.1.
4.4 Special warnings and precautions for use
Asthma
Onbrez Breezhaler is a long-acting beta2-adrenergic agonist, which is only indicated for COPD and should not be used in asthma due to the absence of long-term outcome data in asthma.
Long-acting beta2-adrenergic agonists may increase the risk of asthma-related serious adverse events, including asthma-related deaths, when used for the treatment of asthma.
Hypersensitivity
Immediate hypersensitivity reactions have been reported after administration of Onbrez Breezhaler. If signs suggesting allergic reactions (in particular, difficulties in breathing or swallowing, swelling of tongue, lips and face, urticaria, skin rash) occur, Onbrez Breezhaler should be discontinued immediately and alternative therapy instituted.
Paradoxical bronchospasm
As with other inhalation therapy, administration of Onbrez Breezhaler may result in paradoxical bronchospasm that may be life-threatening. If paradoxical bronchospasm occurs Onbrez Breezhaler should be discontinued immediately and alternative therapy substituted.
Deterioration of disease
Onbrez Breezhaler is not indicated for the treatment of acute episodes of bronchospasm, i.e. as rescue therapy. In the event of deterioration of COPD during treatment with Onbrez Breezhaler, a re-evaluation of the patient and of the COPD treatment regimen should be undertaken. An increase in the daily dose of Onbrez Breezhaler beyond the maximum dose of 300 microgram is not appropriate.
Systemic effects
Although no clinically relevant effect on the cardiovascular system is usually seen after the administration of Onbrez Breezhaler at the recommended doses, as with other beta2-adrenergic agonists, indacaterol should be used with caution in patients with cardiovascular disorders (coronary artery disease, acute myocardial infarction, cardiac arrhythmias, hypertension), in patients with convulsive disorders or thyrotoxicosis, and in patients who are unusually responsive to beta2-adrenergic agonists.
Cardiovascular effects
Like other beta2-adrenergic agonists, indacaterol may produce a clinically significant cardiovascular effect in some patients as measured by increases in pulse rate, blood pressure, and/or symptoms. In case such effects occur, treatment may need to be discontinued. In addition, beta-adrenergic agonists have been reported to produce electrocardiogram (ECG) changes, such as flattening of the T wave, prolongation of QT interval and ST segment depression, although the clinical significance of these observations is unknown. Therefore, long-acting beta2-adrenergic agonists such as Onbrez Breezhaler should be used with caution in patients with known or suspected prolongation of the QT interval or treated with medicinal products affecting the QT interval.
Clinically relevant effects on prolongation of the QTc-interval have not been observed in clinical studies of Onbrez Breezhaler at recommended therapeutic doses (see section 5.1).
Hypokalaemia
Beta2-adrenergic agonists may produce significant hypokalaemia in some patients, which has the potential to produce adverse cardiovascular effects. The decrease in serum potassium is usually transient, not requiring supplementation. In patients with severe COPD, hypokalaemia may be potentiated by hypoxia and concomitant treatment (see section 4.5), which may increase the susceptibility to cardiac arrhythmias.
Hyperglycaemia
Inhalation of high doses of beta2-adrenergic agonists may produce increases in plasma glucose. Upon initiation of treatment with Onbrez Breezhaler plasma glucose should be monitored more closely in diabetic patients.
During clinical studies, clinically notable changes in blood glucose were generally more frequent by 1-2% on Onbrez Breezhaler at the recommended doses than on placebo. Onbrez Breezhaler has not been investigated in patients with not well controlled diabetes mellitus.
4.5 Interaction with other medicinal products and other forms of interaction
Sympathomimetic agents
Concomitant administration of other sympathomimetic agents (alone or as part of combination therapy) may potentiate the undesirable effects of Onbrez Breezhaler.
Onbrez Breezhaler should not be used in conjunction with other long-acting beta2-adrenergic agonists or medicinal products containing long-acting beta2-adrenergic agonists.
Hypokalaemic treatment
Concomitant hypokalaemic treatment with methylxanthine derivatives, steroids, or non-potassium-sparing diuretics may potentiate the possible hypokalaemic effect of beta2-adrenergic agonists, therefore use with caution (see section 4.4).
Beta-adrenergic blockers
Beta-adrenergic blockers and beta2-adrenergic agonists may weaken or antagonise the effect of each other when administered concurrently. Therefore indacaterol should not be given together with beta-adrenergic blockers (including eye drops) unless there are compelling reasons for their use. Where required, cardioselective beta-adrenergic blockers should be preferred, although they should be administered with caution.
Metabolic and transporter based interactions
Inhibition of the key contributors of indacaterol clearance, CYP3A4 and P-glycoprotein (P-gp) raises the systemic exposure of indacaterol by up to two-fold. The magnitude of exposure increases due to interactions does not raise any safety concerns given the safety experience of treatment with Onbrez Breezhaler in clinical studies of up to one year at doses up to twice the maximum recommended therapeutic dose.
Indacaterol has not been shown to cause interactions with co-medications. In vitro investigations have indicated that indacaterol has negligible potential to cause metabolic interactions with medicinal products at the systemic exposure levels achieved in clinical practice.
4.6 Fertility, pregnancy and lactation
Pregnancy
There are no data from the use of indacaterol in pregnant women available. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity at clinically relevant exposures (see section 5.3). Like other beta2-adrenergic agonists, indacaterol may inhibit labour due to a relaxant effect on uterine smooth muscle. Onbrez Breezhaler should only be used during pregnancy if the expected benefits outweigh the potential risks.
Breast-feeding
It is not known whether indacaterol/metabolites are excreted in human milk. Available pharmacokinetic/toxicological data in animals have shown excretion of indacaterol/metabolites in milk (see section 5.3). A risk to the breast-fed child cannot be excluded. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Onbrez Breezhaler therapy, taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
Fertility
A decreased pregnancy rate has been observed in rats. Nevertheless, it is considered unlikely that indacaterol will affect reproductive or fertility performance in humans following inhalation of the maximum recommended dose (see section 5.3).
4.7 Effects on ability to drive and use machines
Onbrez Breezhaler has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable effects
Summary of the safety profile
The most common adverse reactions at the recommended doses were nasopharyngitis (14.3%), upper respiratory tract infection (14.2%), cough (8.2%), headache (3.7%) and muscle spasms (3.5%). These were in the vast majority mild or moderate and became less frequent if treatment was continued.
At the recommended doses, the adverse reaction profile of Onbrez Breezhaler in patients with COPD shows clinically insignificant systemic effects of beta2-adrenergic stimulation. Mean heart rate changes were less than one beat per minute, and tachycardia was infrequent and reported at a similar rate as under placebo treatment. Relevant prolongations of QTcF were not detectable in comparison to placebo. The frequency of notable QTcF intervals [i.e. >450 ms (males) and >470 ms (females)] and reports of hypokalaemia were similar to placebo. The mean of the maximum changes in blood glucose were similar between Onbrez Breezhaler and placebo.
Tabulated summary of adverse reactions
The Onbrez Breezhaler Phase III clinical development programme involved patients with a clinical diagnosis of moderate to severe COPD. 4,764 patients were exposed to indacaterol up to one year at doses up to twice the maximum recommended dose. Of these patients, 2,611 were on treatment with 150 microgram once daily and 1,157 on treatment with 300 microgram once daily. Approximately 41% of patients had severe COPD. The mean age of patients was 64 years, with 48% of patients aged 65 years or older, and the majority (80%) was Caucasian.
Adverse reactions in Table 1 are listed according to MedDRA system organ class in the COPD safety database. Within each system organ class, adverse reactions are ranked by frequency in descending order according to the following convention (CIOMS III): Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data).
Table 1 Adverse reactions
|
Adverse Reactions |
Frequency category |
|
Infections and infestations |
|
Upper respiratory tract infection |
Common |
|
Nasopharyngitis |
Common |
|
Sinusitis |
Common |
|
Immune system disorders |
|
Hypersensitivity1 |
Uncommon |
|
Metabolism and nutrition disorders |
|
Diabetes mellitus and hyperglycaemia |
Uncommon |
|
Nervous system disorders |
|
Headache |
Common |
|
Dizziness |
Common |
|
Paraesthesia |
Uncommon |
|
Cardiac disorders |
|
Ischaemic heart disease |
Uncommon |
|
Atrial fibrillation |
Uncommon |
|
Palpitations |
Uncommon |
|
Tachycardia |
Uncommon |
|
Respiratory, thoracic and mediastinal disorders |
|
Cough |
Common |
|
Oropharyngeal pain including throat irritation |
Common |
|
Rhinorrhoea |
Common |
|
Paradoxical bronchospasm |
Uncommon |
|
Skin and subcutaneous tissue disorders |
|
Pruritus/rash |
Uncommon |
|
Musculoskeletal and connective tissue disorders |
|
Muscle spasm |
Common |
|
Myalgia |
Uncommon |
|
Musculoskeletal pain |
Uncommon |
|
General disorders and administration site conditions |
|
Chest pain |
Common |
|
Peripheral oedema |
Common |
1 Reports of hypersensitivity have been received from post-approval marketing experience in association with the use of Onbrez Breezhaler. These were reported voluntarily from a population of uncertain size, and it is therefore not always possible to reliably estimate the frequency or establish a causal relationship to drug exposure. Therefore the frequency was calculated from clinical trial experience.
At 600 microgram once-daily, the safety profile of Onbrez Breezhaler was overall similar to that of recommended doses. An additional adverse reaction was tremor (common).
Description of selected adverse reactions
In Phase III clinical studies, healthcare providers observed during clinic visits that on average 17-20% of patients experienced a sporadic cough that occurred usually within 15 seconds following inhalation and typically lasted for 5 seconds (about 10 seconds in current smokers). It was observed with a higher frequency in female than in male patients and in current smokers than in ex-smokers. This cough experienced post inhalation was generally well tolerated and did not lead to any patient discontinuing from the studies at the recommended doses (cough is a symptom in COPD and only 8.2% of patients reported cough as an adverse event). There is no evidence that cough experienced post inhalation is associated with bronchospasm, exacerbations, deteriorations of disease or loss of efficacy.
4.9 Overdose
In COPD patients, single doses of 10 times the maximum recommended therapeutic dose were associated with a moderate increase in pulse rate, systolic blood pressure and QTc interval.
An overdose of indacaterol is likely to lead to exaggerated effects typical of beta2-adrenergic stimulants, i.e. tachycardia, tremor, palpitations, headache, nausea, vomiting, drowsiness, ventricular arrhythmias, metabolic acidosis, hypokalaemia and hyperglycaemia.
Supportive and symptomatic treatment is indicated. In serious cases, patients should be hospitalised. Use of cardioselective beta blockers may be considered, but only under the supervision of a physician and with extreme caution since the use of beta-adrenergic blockers may provoke bronchospasm.
5. Pharmacological properties
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Long-acting beta2-adrenergic agonist, ATC code: R03AC18
Mechanism of action
The pharmacological effects of beta2-adrenoceptor agonists are at least in part attributable to stimulation of intracellular adenyl cyclase, the enzyme that catalyses the conversion of adenosine triphosphate (ATP) to cyclic-3', 5'-adenosine monophosphate (cyclic monophosphate). Increased cyclic AMP levels cause relaxation of bronchial smooth muscle. In vitro studies have shown that indacaterol, a long-acting beta2-adrenergic agonist, has more than 24-fold greater agonist activity at beta2-receptors compared to beta1-receptors and 20-fold greater agonist activity compared to beta3-receptors.
When inhaled, indacaterol acts locally in the lung as a bronchodilator. Indacaterol is a partial agonist at the human beta2-adrenergic receptor with nanomolar potency. In isolated human bronchus, indacaterol has a rapid onset of action and a long duration of action.
Although beta2-receptors are the predominant adrenergic receptors in bronchial smooth muscle and beta1-receptors are the predominant receptors in the human heart, there are also beta2-adrenergic receptors in the human heart comprising 10-50% of the total adrenergic receptors. The precise function of beta2-adrenergic receptors in the heart is not known, but their presence raises the possibility that even highly selective beta2-adrenergic agonists may have cardiac effects.
Pharmacodynamic effects
Onbrez Breezhaler, administered once a day at doses of 150 and 300 microgram consistently provided clinically significant improvements in lung function (as measured by the forced expiratory volume in one second, FEV1) over 24 hours across a number of clinical pharmacodynamic and efficacy studies. There was a rapid onset of action within 5 minutes after inhalation, with an increase in FEV1 relative to baseline of 110-160 ml, comparable to the effect of the fast-acting beta2-agonist salbutamol 200 microgram and statistically significantly faster compared to salmeterol/fluticasone 50/500 microgram. Mean peak improvements in FEV1 relative to baseline were 250-330 ml at steady state.
The bronchodilator effect did not depend on the time of dosing, morning or evening.
Onbrez Breezhaler was shown to reduce lung hyperinflation, resulting in increased inspiratory capacity during exercise and at rest, compared to placebo.
Effects on cardiac electrophysiology
A double-blind, placebo- and active (moxifloxacin)-controlled study for 2 weeks in 404 healthy volunteers demonstrated maximum mean (90% confidence intervals) prolongations of the QTcF interval (in milliseconds) of 2.66 (0.55, 4.77) 2.98 (1.02, 4.93) and 3.34 (0.86, 5.82) following multiple doses of 150 microgram, 300 microgram and 600 microgram, respectively. Therefore, this shows no concern for a pro-arrhythmic potential related to QT-interval prolongations at recommended therapeutic doses or at twice the maximum recommended dose. There was no evidence of a concentration-delta QTc relationship in the range of doses evaluated.
As demonstrated in 605 patients with COPD in a 26-week, double-blind, placebo-controlled Phase III study, there was no clinically relevant difference in the development of arrhythmic events monitored over 24 hours, at baseline and up to 3 times during the 26-week treatment period, between patients receiving recommended doses of Onbrez Breezhaler treatment and those patients who received placebo or treatment with tiotropium.
Clinical efficacy and safety
The clinical development programme included one 12-week, two six-month (one of which was extended to one year to evaluate safety and tolerability) and one one-year randomised controlled studies in patients with a clinical diagnosis of COPD. These studies included measures of lung function and of health outcomes such as dyspnoea, exacerbations and health-related quality of life.
Lung function
Onbrez Breezhaler, administered once a day at doses of 150 microgram and 300 microgram, showed clinically meaningful improvements in lung function. At the 12-week primary endpoint (24-hour trough FEV1), the 150 microgram dose resulted in a 130-180 ml increase compared to placebo (p<0.001) and a 60 ml increase compared to salmeterol 50 microgram twice a day (p<0.001). The 300 microgram dose resulted in a 170-180 ml increase compared to placebo (p<0.001) and a 100 ml increase compared to formoterol 12 microgram twice a day (p<0.001). Both doses resulted in an increase of 40-50 ml over open-label tiotropium 18 microgram once a day (150 microgram, p=0.004; 300 microgram, p=0.01). The 24-hour bronchodilator effect of Onbrez Breezhaler was maintained from the first dose throughout a one-year treatment period with no evidence of loss in efficacy (tachyphylaxis).
Symptomatic benefits
Both doses demonstrated statistically significant improvements in symptom relief over placebo for dyspnoea and health status (as evaluated by Transitional Dyspnoea Index [TDI] and St. George's Respiratory Questionnaire [SGRQ], respectively). The magnitude of response was generally greater than seen with active comparators (Table 2). In addition, patients treated with Onbrez Breezhaler required significantly less rescue medication, had more days when no rescue medication was needed compared to placebo and had a significantly improved percentage of days with no daytime symptoms.
Pooled efficacy analysis over 6 months' treatment demonstrated that the rate of COPD exacerbations was statistically significantly lower than the placebo rate. Treatment comparison compared to placebo showed a ratio of rates of 0.68 (95% CI [ 0.47, 0.98]; p-value 0.036) and 0.74 (95% CI [0.56, 0.96]; p-value 0.026) for 150 microgram and 300 microgram, respectively.
Limited treatment experience is available in individuals of African descent.
Table 2 Symptom relief at 6 months treatment duration
|
Treatment Dose (microgram) |
Indacaterol
150
once a day |
Indacaterol
300
once a day |
Tiotropium
18
once a day |
Salmeterol
50
twice a day |
Formoterol
12
twice a day |
Placebo |
|
Percentage of patients who achieved MCID TDI† |
57 a
62 b |
71 b
59 c |
57 b |
54 a |
54 c |
45 a
47 b
41 c |
|
Percentage of patients who achieved MCID SGRQ† |
53 a
58 b |
53 b
55 c |
47 b |
49 a |
51 c |
38 a
46 b
40 c |
|
Reduction in puffs/day of rescue medication use vs. baseline |
1.3 a
1.5 b |
1.6 b |
1.0 b |
1.2 a |
n/e |
0.3 a
0.4 b |
|
Percentage of days with no rescue medication use |
60 a
57 b |
58 b |
46 b |
55 a |
n/e |
42 a
42 b | Study design with a: indacaterol 150 microgram, salmeterol and placebo; b: indacaterol 150 and 300 microgram, tiotropium and placebo; c: indacaterol 300 microgram, formoterol and placebo
† MCID = minimal clinically important difference (≥1 point change in TDI, ≥4 point change in SGRQ)
n/e= not evaluated at six months
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with Onbrez Breezhaler in all subsets of the paediatric population in chronic obstructive pulmonary disease (COPD) (see section 4.2 for information on paediatric use).
5.2 Pharmacokinetic properties
Indacaterol is a chiral molecule with R-configuration.
Pharmacokinetic data were obtained from a number of clinical studies, from healthy volunteers and COPD patients.
Absorption
The median time to reach peak serum concentrations of indacaterol was approximately 15 min after single or repeated inhaled doses. Systemic exposure to indacaterol increased with increasing dose (150 microgram to 600 microgram) in a dose proportional manner. Absolute bioavailability of indacaterol after an inhaled dose was on average 43% to 45%. Systemic exposure results from a composite of pulmonary and gastrointestinal absorption; about 75% of systemic exposure was from pulmonary absorption and about 25% from gastrointestinal absorption.
Indacaterol serum concentrations increased with repeated once-daily administration. Steady state was achieved within 12 to 14 days. The mean accumulation ratio of indacaterol, i.e. AUC over the 24-h dosing interval on Day 14 compared to Day 1, was in the range of 2.9 to 3.5 for once-daily inhaled doses between 150 microgram and 600 microgram.
Distribution
After intravenous infusion the volume of distribution of indacaterol during the terminal elimination phase was 2557 litres indicating an extensive distribution. The in vitro human serum and plasma protein binding was 94.1-95.3% and 95.1-96.2%, respectively.
Biotransformation
After oral administration of radiolabelled indacaterol in a human ADME (absorption, distribution, metabolism, excretion) study, unchanged indacaterol was the main component in serum, accounting for about one third of total drug-related AUC over 24 hours. A hydroxylated derivative was the most prominent metabolite in serum. Phenolic O-glucuronides of indacaterol and hydroxylated indacaterol were further prominent metabolites. A diastereomer of the hydroxylated derivative, a N-glucuronide of indacaterol, and C- and N-dealkylated products were further metabolites identified.
In vitro investigations indicated that UGT1A1 is the only UGT isoform that metabolised indacaterol to the phenolic O-glucuronide. The oxidative metabolites were found in incubations with recombinant CYP1A1, CYP2D6, and CYP3A4. CYP3A4 is concluded to be the predominant isoenzyme responsible for hydroxylation of indacaterol. In vitro investigations further indicated that indacaterol is a low affinity substrate for the efflux pump P-gp.
Elimination
In clinical studies which included urine collection, the amount of indacaterol excreted unchanged via urine was generally lower than 2% of the dose. Renal clearance of indacaterol was, on average, between 0.46 and 1.20 litres/hour. When compared with the serum clearance of indacaterol of 23.3 litres/hour, it is evident that renal clearance plays a minor role (about 2 to 5% of systemic clearance) in the elimination of systemically available indacaterol.
In a human ADME study where indacaterol was given orally, the faecal route of excretion was dominant over the urinary route. Indacaterol was excreted into human faeces primarily as unchanged parent substance (54% of the dose) and, to a lesser extent, hydroxylated indacaterol metabolites (23% of the dose). Mass balance was complete with ≥90% of the dose recovered in the excreta.
Indacaterol serum concentrations declined in a multi-phasic manner with an average terminal half-life ranging from 45.5 to 126 hours. The effective half-life, calculated from the accumulation of indacaterol after repeated dosing ranged from 40 to 52 hours which is consistent with the observed time-to-steady state of approximately 12-14 days.
Special populations
A population pharmacokinetic analysis showed that there is no clinically relevant effect of age (adults up to 88 years), sex, weight (32-168 kg) or race on the pharmacokinetics of indacaterol. It did not suggest any difference between ethnic subgroups in this population.
Patients with mild and moderate hepatic impairment showed no relevant changes in Cmax or AUC of indacaterol, nor did protein binding differ between mild and moderate hepatic impaired subjects and their healthy controls. Studies in subjects with severe hepatic impairment were not performed.
Due to the very low contribution of the urinary pathway to total body elimination, a study in renally impaired subjects was not performed.
5.3 Preclinical safety data
Effects on the cardiovascular system attributable to the beta2-agonistic properties of indacaterol included tachycardia, arrhythmias and myocardial lesions in dogs. Mild irritancy of the nasal cavity and larynx were seen in rodents. All these findings occurred at exposures sufficiently in excess of those anticipated in humans.
Although indacaterol did not affect general reproductive performance in a rat fertility study, a decrease in the number of pregnant F1 offspring was observed in the peri- and post-developmental rat study at an exposure 14-fold higher than in humans treated with Onbrez Breezhaler. Indacaterol was not embryotoxic or teratogenic in rats or rabbits.
Genotoxicity studies did not reveal any mutagenic or clastogenic potential. Carcinogenicity was assessed in a two-year rat study and a six-month transgenic mouse study. Increased incidences of benign ovarian leiomyoma and focal hyperplasia of ovarian smooth muscle in rats were consistent with similar findings reported for other beta2-adrenergic agonists. No evidence of carcinogenicity was seen in mice. Systemic exposures (AUC) in rats and mice at the no-observed adverse effect levels in these studies were at least 7- and 49-fold higher, respectively, than in humans treated with Onbrez Breezhaler once a day at a dose of 300 microgram.
6. Pharmaceutical particulars
6.1 List of excipients
Capsule content
Lactose monohydrate
Capsule shell
Gelatin
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years.
6.4 Special precautions for storage
Do not store above 30°C.
Onbrez Breezhaler capsules must always be stored in the blister to protect from moisture and only removed immediately before use.
6.5 Nature and contents of container
Onbrez Breezhaler is a single-dose inhalation device. Inhaler body and cap are made from acrylonitrile butadiene styrene, push buttons are made from methyl methacrylate acrylonitrile butadiene styrene. Needles and springs are made from stainless steel.
PA/Alu/PVC - Alu blister packs, containing 10 hard capsules, with an inhaler made from plastic materials provided in each pack.
Carton containing 10 capsules (1x10 capsule blister strips) and one Onbrez Breezhaler inhaler.
Carton containing 30 capsules (3x10 capsule blister strips) and one Onbrez Breezhaler inhaler.
Multipack comprising 2 packs (each containing 30 capsules and 1 inhaler).
Multipack comprising 3 packs (each containing 30 capsules and 1 inhaler).
Multipack comprising 30 packs (each containing 10 capsules and 1 inhaler).
Not all pack sizes may be marketed.
6.6 Special precautions for disposal and other handling
The Onbrez Breezhaler inhaler provided with each new prescription should be used. Dispose of each inhaler after 30 days of use.
Instructions for handling and use
Pull off the cap.

Open inhaler:
Hold the base of the inhaler firmly and tilt the mouthpiece. This opens the inhaler.

Prepare capsule:
Immediately before use, with dry hands, remove one capsule from the blister.
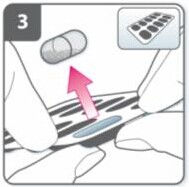
Insert capsule:
Place the capsule into the capsule chamber.
Never place a capsule directly into the mouthpiece.

Close the inhaler:
Close the inhaler until you hear a “click”.

Pierce the capsule:
• Hold the inhaler upright with the mouthpiece pointing up.
• Pierce the capsule by firmly pressing together both side buttons at the same time. Do this only once.
• You should hear a “click” as the capsule is being pierced.

Release the side buttons fully.

Breathe out:
Before placing the mouthpiece in your mouth, breathe out fully.
Do not blow into the mouthpiece.

Inhale the medicine
To breathe the medicine deeply into your airways:
• Hold the inhaler as shown in the picture. The side buttons should be facing left and right. Do not press the side buttons.
• Place the mouthpiece in your mouth and close your lips firmly around it.
• Breathe in rapidly but steadily and as deeply as you can.

Note:
As you breathe in through the inhaler, the capsule spins around in the chamber and you should hear a whirring noise. You will experience a sweet flavour as the medicine goes into your lungs.
Additional information
Occasionally, very small pieces of the capsule can get past the screen and enter your mouth. If this happens, you may be able to feel these pieces on your tongue. It is not harmful if these pieces are swallowed or inhaled. The chances of the capsule shattering will be increased if the capsule is accidentally pierced more than once (step 6).
If you do not hear a whirring noise:
The capsule may be stuck in the capsule chamber. If this happens:
• Open the inhaler and carefully loosen the capsule by tapping the base of the inhaler. Do not press the side buttons.
• Inhale the medicine again by repeating steps 8 and 9.

Hold breath:
After you have inhaled the medicine:
• Hold your breath for at least 5-10 seconds or as long as you comfortably can while taking the inhaler out of your mouth.
• Then breathe out.
• Open the inhaler to see if any powder is left in the capsule.
If there is powder left in the capsule:
• Close the inhaler.
• Repeat steps 8, 9, 10 and 11.
Most people are able to empty the capsule with one or two inhalations.
Additional information
Some people may occasionally cough briefly soon after inhaling the medicine. If you do, don't worry. As long as the capsule is empty, you have received enough of your medicine.

After you have finished taking your medicine:
• Open the mouthpiece again, and remove the empty capsule by tipping it out of the capsule chamber. Put the empty capsule in your household waste.
• Close the inhaler and replace the cap.
Do not store the capsules in the Onbrez Breezhaler inhaler.

Mark daily dose tracker:
On the inside of the pack there is a daily dose tracker. Put a mark in today's box if it helps to remind you of when your next dose is due.

7. Marketing authorisation holder
Novartis Europharm Limited
Wimblehurst Road
Horsham
West Sussex, RH12 5AB
United Kingdom
8. Marketing authorisation number(s)
Onbrez Breezhaler 150 microgram inhalation powder, hard capsules: EU/1/09/593/001-005
Onbrez Breezhaler 300 microgram inhalation powder, hard capsules: EU/1/09/593/006-010
9. Date of first authorisation/renewal of the authorisation
30.11.2009
10. Date of revision of the text
16.12.2013
Detailed information on this medicinal product is available on the website of the European Medicines Agency http://www.ema.europa.eu
---------------------------------------------------------
包括规格
30粒x150ug
90粒x150ug
30粒x300ug
90粒x300ug |
